Respiratory System MCQs for pharmacist exams
Practice Respiratory System MCQs for pharmacist exams with answers and explanations for GPAT, NIPER, AIIMS Pharmacist, SSC, ESIC, Railway, HSSC, and State Pharmacist exams.
Dr. Alok Singh
7/5/202611 min read
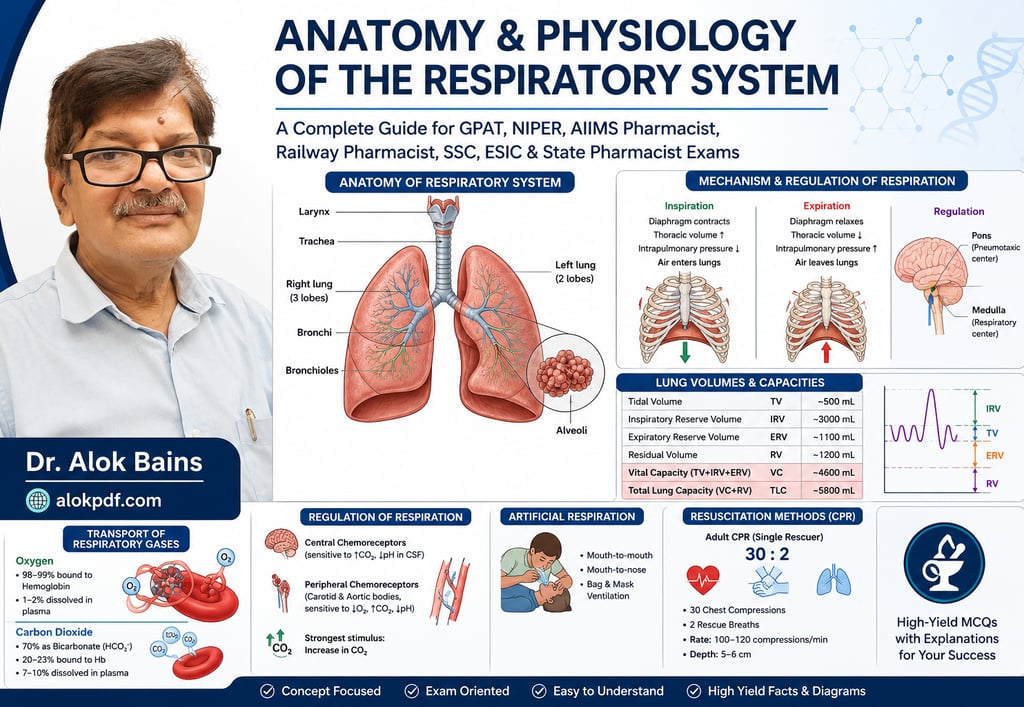
MCQs on Anatomy and Physiology of the Respiratory System for GPAT, NIPER, AIIMS Pharmacist, Railway Pharmacist, SSC, ESIC, and State Pharmacist Exams.
Quick Revision
These short notes summarize the most frequently tested concepts and numerical values from the respiratory system. Revise them before attempting the MCQs.
1. Functions of the Respiratory System
Supplies oxygen (O₂) to tissues.
Removes carbon dioxide (CO₂) from the body.
Maintains acid-base balance by regulating blood CO₂.
Produces voice (phonation).
Enables the sense of smell (olfaction).
Filters, warms, and humidifies inspired air.
Exam Tip: The primary function of respiration is gas exchange, not oxygen transport.
2. Conducting Zone vs Respiratory Zone
Conducting Zone
Nose
Nasal cavity
Pharynx
Larynx
Trachea
Bronchi
Bronchioles
Terminal bronchioles
Function: Conducts air only (no gas exchange).
Respiratory Zone
Respiratory bronchioles
Alveolar ducts
Alveolar sacs
Alveoli
Function: Gas exchange occurs.
Remember: Gas exchange begins at the respiratory bronchioles.
3. Anatomy of the Lungs
Right Lung Left Lung
3 lobes 2 lobes
Horizontal & oblique fissures Oblique fissure only
Larger and heavier Smaller because of heart
10 bronchopulmonary segments 8–10 bronchopulmonary segments
More vertical bronchus Less vertical bronchus
Most Important Fact: Aspirated foreign bodies usually enter the right main bronchus.
4. Alveoli
Functional unit of the lungs.
About 300 million alveoli in both lungs.
Surface area ≈ 70 m².
Thin respiratory membrane allows rapid diffusion.
Alveolar Cells
Type I Pneumocytes
Gas exchange
Cover about 95% of alveolar surface
Type II Pneumocytes
Produce surfactant
Repair damaged alveoli
Alveolar Macrophages
Remove dust and microorganisms.
Remember: Type I = Gas exchange; Type II = Surfactant.
5. Pulmonary Surfactant
Produced by Type II pneumocytes.
Functions
Reduces surface tension.
Prevents alveolar collapse (atelectasis).
Increases lung compliance.
Reduces work of breathing.
Clinical Pearl: Surfactant deficiency causes Respiratory Distress Syndrome in premature infants.
6. Mechanism of Respiration
Inspiration (Active)
The diaphragm contracts.
External intercostals contract.
Thoracic cavity volume increases.
Intrapulmonary pressure decreases.
Air enters lungs.
Expiration (Passive)
Diaphragm relaxes.
Elastic recoil of lungs.
Thoracic volume decreases.
Intrapulmonary pressure increases.
Air leaves lungs.
Easy Trick
Inspiration = Muscle contraction + Volume ↑ + Pressure ↓ + Air enters
7. Muscles of Respiration
Quiet Inspiration
Diaphragm (major muscle)
External intercostals
Forced Inspiration
Sternocleidomastoid
Scalene muscles
Forced Expiration
Internal intercostals
Abdominal muscles
Remember: Quiet expiration requires no muscle contraction.
8. Lung Volumes
Volume Normal Value
Tidal Volume (TV) 500 mL
Inspiratory Reserve Volume (IRV) 3000 mL
Expiratory Reserve Volume (ERV) 1100 mL
Residual Volume (RV) 1200 mL
Frequently Asked: Residual volume cannot be measured by simple spirometry.
9. Lung Capacities
Capacity Formula
Inspiratory Capacity TV + IRV
Functional Residual Capacity ERV + RV
Vital Capacity TV + IRV + ERV
Total Lung Capacity VC + RV
Easy Trick
Vital Capacity = All movable air
Residual Volume = Air that never leaves the lungs
10. Transport of Oxygen
98–99% transported bound to hemoglobin.
1–2% dissolved in plasma.
Remember: Hemoglobin is the major oxygen carrier.
11. Transport of Carbon Dioxide
Form Percentage
Bicarbonate (HCO₃⁻) 70%
Carbaminohemoglobin 20–23%
Dissolved in plasma 7–10%
High-Yield Enzyme
Carbonic anhydrase catalyzes the conversion of CO₂ to bicarbonate in RBCs.
12. Regulation of Respiration
Respiratory Centers
Medulla oblongata → Basic respiratory rhythm.
Pons → Modifies respiratory rhythm.
Chemoreceptors
Central Chemoreceptors
Respond mainly to increased CO₂ (via H⁺ in CSF).
Peripheral Chemoreceptors
Located in carotid and aortic bodies.
Respond mainly to decreased O₂.
Exam Favourite: Normal respiration is primarily regulated by CO₂, not O₂.
13. Artificial Respiration
Methods include:
Mouth-to-mouth.
Mouth-to-nose.
Bag-valve-mask ventilation.
Mechanical ventilator.
Purpose: Maintain oxygenation until spontaneous breathing resumes.
14. Cardiopulmonary Resuscitation (CPR)
Adult CPR
Compression : Ventilation = 30 : 2
Compression rate = 100–120/min
Compression depth = 5–6 cm
Allow complete chest recoil.
Remember: Push hard, push fast, minimize interruptions.
15. Frequently Asked Numerical Values
Right lung = 3 lobes
Left lung = 2 lobes
Tidal volume = 500 mL
Residual volume = 1200 mL
Vital capacity ≈ 4600 mL
Total lung capacity ≈ 5800–6000 mL
Adult respiratory rate = 12–20 breaths/min
Last-Minute Revision
Gas exchange begins in respiratory bronchioles.
The right main bronchus is the common site for aspiration.
Type I pneumocytes: Gas exchange.
Type II pneumocytes: Surfactant secretion.
Quiet inspiration is active.
Quiet expiration is passive.
Surfactant decreases surface tension and prevents alveolar collapse.
CO₂ is the strongest physiological stimulus for respiration.
Residual volume cannot be measured by spirometry.
Vital Capacity = TV + IRV + ERV.
Total Lung Capacity = VC + RV.
70% of CO₂ is transported as bicarbonate.
98–99% of O₂ is transported by hemoglobin.
Adult CPR = 30 compressions: 2 breaths at 100–120 compressions/min.
1. The functional unit of the lung responsible for gas exchange is:
A. Bronchiole
B. Trachea
C. Alveolus
D. Pleura
Answer: C. Alveolus
Explanation: Alveoli are the primary sites of gaseous exchange. Their thin walls and extensive capillary network facilitate diffusion of oxygen and carbon dioxide.
2. The right lung is divided into:
A. Two lobes
B. Three lobes
C. Four lobes
D. Five lobes
Answer: B. Three lobes
Explanation: The right lung has superior, middle, and inferior lobes separated by horizontal and oblique fissures.
3. The left lung contains:
A. Three lobes
B. Four lobes
C. Two lobes and a cardiac notch
D. One lobe
Answer: C. Two lobes and a cardiac notch
Explanation: The left lung has superior and inferior lobes. The cardiac notch accommodates the heart.
4. Which cartilage forms the "Adam's apple"?
A. Cricoid cartilage
B. Thyroid cartilage
C. Arytenoid cartilage
D. Epiglottis
Answer: B. Thyroid cartilage
Explanation: The thyroid cartilage is the largest laryngeal cartilage and forms the laryngeal prominence.
5. The conducting zone of the respiratory tract ends at:
A. Alveolar sacs
B. Terminal bronchioles
C. Respiratory bronchioles
D. Alveoli
Answer: B. Terminal bronchioles
Explanation: The conducting zone transports air without gas exchange. Gas exchange begins in the respiratory bronchioles.
6. The trachea bifurcates into the primary bronchi at the level of:
A. T4–T5 vertebrae (Sternal angle)
B. T1 vertebra
C. T10 vertebra
D. L1 vertebra
Answer: A. T4–T5 vertebrae (Sternal angle)
Explanation: The tracheal bifurcation (carina) is located at the sternal angle opposite the T4–T5 vertebrae.
7. Which bronchus is more likely to receive an aspirated foreign body?
A. Left main bronchus
B. Right main bronchus
C. Both equally
D. Segmental bronchi
Answer: B. Right main bronchus
Explanation: The right main bronchus is shorter, wider, and more vertical, making aspiration more common.
8. The muscle primarily responsible for quiet inspiration is:
A. Internal intercostals
B. External intercostals
C. Diaphragm
D. Abdominal muscles
Answer: C. Diaphragm
Explanation: Diaphragmatic contraction increases thoracic volume, producing inspiration.
9. During quiet expiration:
A. The diaphragm contracts
B. Internal intercostals contract
C. It is an active process
D. It is mainly passive
Answer: D. It is mainly passive
Explanation: Quiet expiration results from elastic recoil of the lungs and chest wall.
10. Which respiratory muscle is mainly involved in forced expiration?
A. Diaphragm
B. Sternocleidomastoid
C. Internal intercostals and abdominal muscles
D. Scalene muscles
Answer: C. Internal intercostals and abdominal muscles
Explanation: These muscles decrease thoracic volume during forceful expiration.
11. The normal tidal volume in an adult is approximately:
A. 150 mL
B. 250 mL
C. 500 mL
D. 1000 mL
Answer: C. 500 mL
Explanation: Tidal volume is the amount of air inspired or expired during normal breathing.
12. Inspiratory reserve volume (IRV) is approximately:
A. 300 mL
B. 500 mL
C. 1100 mL
D. 3000 mL
Answer: D. 3000 mL
Explanation: IRV is the additional air inspired after a normal inspiration.
13. The expiratory reserve volume (ERV) is approximately:
A. 1200 mL
B. 1100 mL
C. 500 mL
D. 3000 mL
Answer: B. 1100 mL
Explanation: ERV is the maximum extra air expired after normal expiration.
14. Residual volume (RV) is:
A. Air remaining after maximal expiration
B. Air inspired during normal breathing
C. Maximum inspired air
D. Air exchanged during exercise
Answer: A. Air remaining after maximal expiration
Explanation: Residual volume prevents alveolar collapse and cannot be measured by simple spirometry.
15. Vital capacity equals:
A. TV + IRV + ERV
B. TV + RV
C. RV + TLC
D. IRV + RV
Answer: A. TV + IRV + ERV
Explanation: Vital capacity represents the maximum amount of air exhaled after maximum inspiration.
16. Total lung capacity is:
A. VC + RV
B. TV + ERV
C. TV + RV
D. IRV + ERV
Answer: A. VC + RV
Explanation: TLC is the total volume of air in the lungs after maximal inspiration.
17. Which lung volume cannot be measured by simple spirometry?
A. TV
B. IRV
C. ERV
D. RV
Answer: D. RV
Explanation: Residual volume remains in the lungs after maximal expiration and requires special methods.
18. Most oxygen in blood is transported
A. Dissolved in plasma
B. Bound to hemoglobin
C. As bicarbonate
D. Bound to albumin
Answer: B. Bound to hemoglobin
Explanation: About 98–99% of oxygen is transported as oxyhemoglobin.
19. Most carbon dioxide is transported as
A. Carbaminohemoglobin
B. Dissolved gas
C. Bicarbonate ions
D. Carbonic acid
Answer: C. Bicarbonate ions
Explanation: Approximately 70% of CO₂ is transported as bicarbonate in plasma.
20. The enzyme responsible for the rapid conversion of CO₂ into bicarbonate is:
A. Pepsin
B. Carbonic anhydrase
C. Catalase
D. Lipase
Answer: B. Carbonic anhydrase
Explanation: Carbonic anhydrase is present in RBCs and accelerates CO₂ hydration.
21. The respiratory center is primarily located in the:
A. Cerebellum
B. Medulla oblongata and pons
C. Hypothalamus
D. Cerebral cortex
Answer: B. Medulla oblongata and pons
Explanation: The medulla generates respiratory rhythm, while the pons modifies it.
22. The strongest stimulus for respiration under normal conditions is:
A. Increased oxygen concentration
B. Increased carbon dioxide concentration
C. Increased nitrogen concentration
D. Decreased hemoglobin
Answer: B. Increased carbon dioxide concentration
Explanation: Elevated arterial CO₂ increases H⁺ concentration in CSF, stimulating respiration.
23. Peripheral chemoreceptors are located in the:
A. Medulla only
B. Carotid and aortic bodies
C. Cerebral cortex
D. Pulmonary veins
Answer: B. Carotid and aortic bodies
Explanation: These receptors respond mainly to hypoxia and also to hypercapnia and acidosis.
24. Central chemoreceptors respond primarily to:
A. Oxygen levels
B. Carbon dioxide-induced changes in CSF pH
C. Blood pressure
D. Temperature
Answer: B. Carbon dioxide-induced changes in CSF pH
Explanation: Central chemoreceptors are highly sensitive to changes in hydrogen ion concentration resulting from CO₂.
25. During vigorous exercise, ventilation increases mainly because of:
A. Decreased oxygen only
B. Neural stimulation and increased CO₂ production
C. Increased nitrogen
D. Increased plasma proteins
Answer: B. Neural stimulation and increased CO₂ production
Explanation: Both neural input and increased metabolic activity stimulate ventilation.
26. Artificial respiration is mainly intended to:
A. Reduce heart rate
B. Maintain ventilation until spontaneous breathing resumes
C. Increase blood pressure only
D. Stop chest movement
Answer: B. Maintain ventilation until spontaneous breathing resumes
Explanation: Artificial respiration supplies oxygen and removes carbon dioxide when spontaneous breathing has ceased.
27. The recommended compression-to-ventilation ratio during adult CPR (single rescuer) is:
A. 15: 2
B. 20: 2
C. 30: 2
D. 5:1
Answer: C. 30: 2
Explanation: Current CPR guidelines recommend 30 chest compressions followed by 2 rescue breaths for a single rescuer.
28. The recommended chest compression rate during adult CPR is approximately:
A. 40–60/min
B. 60–80/min
C. 100–120/min
D. 140–160/min
Answer: C. 100–120/min
Explanation: Effective compressions should be delivered at 100–120 per minute with adequate depth and recoil.
29. Which of the following increases during inspiration?
A. Intrapulmonary pressure
B. Intra-alveolar pressure above atmospheric pressure
C. Thoracic cavity volume
D. Pleural pressure becomes positive
Answer: C. Thoracic cavity volume
Explanation: Expansion of the thoracic cavity lowers intrapulmonary pressure, allowing air to enter.
30. Which statement regarding surfactant is correct?
A. Produced by Type I pneumocytes
B. Reduces alveolar surface tension
C. Increases alveolar collapse
D. Secreted by alveolar macrophages
Answer: B. Reduces alveolar surface tension
Explanation: Pulmonary surfactant, secreted by Type II pneumocytes, prevents alveolar collapse and decreases the work of breathing.
31. A foreign body accidentally enters the respiratory tract while a person is talking. It is most likely to lodge in the:
A. Left primary bronchus because it is narrower
B. Right primary bronchus because it is wider and more vertical
C. Trachea because it is the largest airway
D. Respiratory bronchioles because they have the smallest diameter
Answer: B. Right primary bronchus because it is wider and more vertical
Explanation: The right main bronchus is shorter, wider, and more vertical than the left, making it the commonest site for aspiration.
32. Which one of the following changes occurs first during normal inspiration?
A. Air enters the lungs.
B. Intrapulmonary pressure falls below atmospheric pressure.
C. Diaphragm contracts.
D. Oxygen diffuses into pulmonary capillaries.
Answer: C. Diaphragm contracts.
Explanation: Contraction of the diaphragm increases thoracic volume, lowering intrapleural and then intrapulmonary pressure, allowing air to enter.
33. A patient has complete paralysis of the diaphragm but intact intercostal muscles. Which respiratory function will be affected the most?
A. Quiet inspiration
B. Forced expiration
C. Gas diffusion
D. Carbon dioxide transport
Answer: A. Quiet inspiration
Explanation: The diaphragm contributes about 70–75% of quiet inspiration. Intercostal muscles alone cannot maintain normal tidal breathing.
34. Which lung volume increases significantly in obstructive lung diseases such as emphysema?
A. Tidal volume
B. Inspiratory reserve volume
C. Residual volume
D. Expiratory reserve volume
Answer: C. Residual volume
Explanation: Air trapping prevents complete expiration, increasing residual volume.
35. A student performs spirometry correctly. Which of the following values cannot be measured directly?
A. Vital capacity
B. Tidal volume
C. Residual volume
D. Inspiratory capacity
Answer: C. Residual volume
Explanation: Residual volume remains in the lungs after maximal expiration and is not measurable by simple spirometry.
36. Which statement best explains why alveoli do not collapse after every expiration?
A. Alveoli contain cartilage.
B. Surfactant reduces surface tension.
C. Oxygen pressure remains high.
D. Carbon dioxide maintains alveolar volume.
Answer: B. Surfactant reduces surface tension.
Explanation: Pulmonary surfactant decreases surface tension, stabilizing alveoli and preventing collapse.
37. If carbonic anhydrase activity is completely inhibited, the immediate consequence would be:
A. Oxygen transport stops.
B. Carbon dioxide transport becomes slower.
C. Hemoglobin synthesis decreases.
D. Lung compliance increases.
Answer: B. Carbon dioxide transport becomes slower.
Explanation: Carbonic anhydrase catalyzes rapid conversion of CO₂ to bicarbonate inside RBCs.
38. Which factor provides the greatest stimulus for breathing in a healthy individual?
A. Low oxygen concentration
B. High carbon dioxide concentration
C. Increased hemoglobin concentration
D. Increased bicarbonate concentration
Answer: B. High carbon dioxide concentration
Explanation: Under normal physiological conditions, increased arterial PCO₂ is the strongest respiratory stimulus.
39. During forced expiration, which statement is correct?
A. It occurs entirely due to elastic recoil.
B. Diaphragm contracts forcefully.
C. Internal intercostals and abdominal muscles contract.
D. External intercostals are the primary muscles.
Answer: C. Internal intercostals and abdominal muscles contract.
Explanation: Forced expiration is an active process involving contraction of expiratory muscles.
40. Which statement regarding oxygen transport is MOST accurate?
A. Most oxygen is dissolved in plasma.
B. Oxygen binds mainly to plasma proteins.
C. Most oxygen is transported bound to hemoglobin.
D. Oxygen is transported mainly as bicarbonate.
Answer: C. Most oxygen is transported bound to hemoglobin.
Explanation: Approximately 98–99% of oxygen is carried as oxyhemoglobin.
41. During vigorous exercise, arterial oxygen saturation usually remains nearly normal because:
A. Hemoglobin concentration doubles.
B. Ventilation increases to match metabolic demand.
C. Carbon dioxide production decreases.
D. Diffusion distance decreases.
Answer: B. Ventilation increases to match metabolic demand.
Explanation: Increased ventilation maintains arterial oxygen despite increased oxygen consumption.
42. Which of the following events occurs during expiration?
A. Thoracic volume increases.
B. Intrapulmonary pressure becomes lower than atmospheric pressure.
C. Elastic recoil of lungs predominates.
D. Diaphragm contracts.
Answer: C. Elastic recoil of lungs predominates.
Explanation: Quiet expiration is mainly passive due to elastic recoil.
43. Which combination correctly represents Vital Capacity?
A. TV + RV
B. TV + IRV + ERV
C. TV + RV + ERV
D. TLC − IRV
Answer: B. TV + IRV + ERV
Explanation: Vital capacity is the maximum volume expelled after maximal inspiration.
44. A patient has damage to the medulla oblongata while the pons remains intact. Which function is most likely to be severely affected?
A. Regulation of body temperature
B. Generation of respiratory rhythm
C. Vision
D. Hearing
Answer: B. Generation of respiratory rhythm
Explanation: The medullary respiratory center generates the basic respiratory rhythm.
45. Which statement about Type II pneumocytes is FALSE?
A. They produce surfactant.
B. They reduce surface tension.
C. They are involved in alveolar repair.
D. They are the principal site of gas exchange.
Answer: D. They are the principal site of gas exchange.
Explanation: Gas exchange mainly occurs through Type I pneumocytes.
46. If surfactant were suddenly absent, which of the following would occur first?
A. Increased lung compliance
B. Alveolar collapse
C. Increased oxygen transport
D. Increased tidal volume
Answer: B. Alveolar collapse
Explanation: Loss of surfactant markedly increases surface tension, causing atelectasis.
47. During CPR, rescue breaths are given mainly to:
A. Increase venous return
B. Maintain alveolar ventilation
C. Increase coronary blood flow
D. Raise arterial pressure
Answer: B. Maintain alveolar ventilation
Explanation: Rescue breaths provide oxygen and eliminate carbon dioxide until spontaneous breathing returns.
48. Which statement best distinguishes anatomical dead space from alveolar dead space?
A. Anatomical dead space participates in gas exchange.
B. Alveolar dead space consists of conducting airways.
C. Anatomical dead space contains no alveoli.
D. Anatomical dead space contains only alveoli.
Answer: C. Anatomical dead space contains no alveoli.
Explanation: Conducting airways (nose to terminal bronchioles) constitute anatomical dead space.
49. Which sequence correctly describes normal inspiration?
A. Air enters: diaphragm contracts: thoracic volume increases
B. Diaphragm contracts: Thoracic volume increases: intrapulmonary pressure falls: air enters lungs
C. Thoracic volume decreases: pressure falls: air enters
D. Pressure rises: diaphragm contracts: air enters
Answer: B. Diaphragm contracts: thoracic volume increases: intrapulmonary pressure falls: air enters lungs
Explanation: This is the correct physiological sequence of inspiration.
50. Which of the following statements is CORRECT regarding carbon dioxide transport?
A. Most CO₂ is transported bound to hemoglobin.
B. Most CO₂ is dissolved in plasma.
C. Most CO₂ is transported as bicarbonate ions.
D. CO₂ is transported only inside RBCs.
Answer: C. Most CO₂ is transported as bicarbonate ions.
Explanation: Approximately 70% of CO₂ is transported as bicarbonate in plasma after formation inside RBCs.
Remember for the exam
Remember the sequence: Muscle contraction → Volume ↑ → Pressure ↓ → Air enters.
Right bronchus: Wider, shorter, more vertical → aspiration.
Surfactant: ↓ Surface tension → ↑ Lung compliance → Prevents alveolar collapse.
CO₂ is the chief regulator of respiration under normal conditions.
Residual volume cannot be measured by spirometry.
Type I pneumocytes: Gas exchange.
Type II pneumocytes: Surfactant secretion and alveolar repair.
Quiet inspiration: Active.
Quiet expiration: Passive.
Forced expiration: Active (internal intercostals + abdominal muscles).
One-Liners for Competitive Examinations
Right lung: 3 lobes, 10 bronchopulmonary segments.
Left lung: 2 lobes, cardiac notch, and lingula.
Functional unit: Alveolus.
Gas exchange membrane thickness: Approximately 0.5 μm.
Normal tidal volume: 500 mL.
Vital capacity = TV + IRV + ERV.
Total lung capacity = VC + RV.
Residual volume cannot be measured by simple spirometry.
98–99% of oxygen is transported by hemoglobin.
70% of CO₂ is transported as bicarbonate ions.
Carbonic anhydrase is present in RBCs.
Primary respiratory center: Medulla oblongata.
Pneumotaxic center: Limits inspiration.
Apneustic center: Prolongs inspiration.
Central chemoreceptors: respond mainly to CO₂.
Peripheral chemoreceptors: respond mainly to low arterial O₂.
Quiet inspiration: Active process.
Quiet expiration: Passive process.
Type II pneumocytes: Produce surfactant.
Right main bronchus: Common site for aspiration.
Adult CPR: 30 compressions: 2 breaths; compression rate 100–120/min.
Dr. Alok Simgh